Transforming hematopoietic stem cell transplantation

Interview with Alain Vertès (Sloan Fellow, London Business School: Managing Director, NxR Biotechnologies GmbH, Basel, Switzerland), on the cell therapy industry and how it may offer potential for improved hematologic reconstitution and reducing graft-versus-host disease
Hematopoietic stem cell transplantation (HSCT) is a life-saving treatment for indications such as inherited anemias, immune deficiencies and hematologic malignancies. However, allogeneic HSCT comes with a high price: graft-versus-host disease (GVHD), where the donor’s immune cells attack the tissues of the recipient and occurs in 40—60% of allogeneic transplantation patients resulting in significant morbidity and mortality. Therefore, improved GVHD treatments are needed to increase survival rates of those with GVHD, without reducing the efficacy of the original stem cell transplant.
In this interview Alain Vertès discusses the cell therapy industry and the potential of cytotherapeutics in hematologic reconstitution and in the treatment and prophylaxis of GVHD, following on from the recent publication of two Regenerative Medicine review articles on the topic, written by Alain.

Alain Vertès, PhD, MBA, is managing director of Basel, Switzerland-based NxR Biotechnologies, a consultancy that assists companies in funding, positioning and commercializing biotech products. He is an active business development consultant focused on technology deployment, and innovation funding and commercialization. He has contributed to research (molecular biology, microbiology, sustainable chemistry), manufacturing (amino acids, enzymes), contract research (Battelle Memorial Institute, PPD), and strategic alliances in pharmaceuticals (Roche, Pfizer, Lilly), biotech (Mesoblast, Targazyme), petrochemicals (Mitsubishi Chemical Corp.), industrial biotechnology, public research and consulting. With worldwide experience in partnering and licensing groups of big pharmas and biotechs, Vertès has led reviews of strategic needs for finding, implementing and managing partnerships, from licensing to M&As. With hands-on involvement in the deployment of radical innovation-for example, bringing to patients disease-modifying, paradigm-changing therapeutics, he has managed major siRNA and regenerative medicine alliances, and has led global therapeutic stem cell initiatives.
You have recently written about the current practice of HSCT and potential technologies that may offer future clinical benefits. Can you tell us a bit about your interest in HSCT?
There are reasons to believe that stem cell technologies will work, as we already have an outstanding example with HSCT. HSCT has already been performed for over 50 years, so there is a long history of using stem cells as a therapy already. 50 years of HSCT has saved lives: stem cells save lives. It’s important we advocate the technology of therapeutic stem cells as products derived from these cells have such great potential.
“It’s important we advocate the technology of therapeutic stem cells as products derived from these cells have such great potential.”
Owing to the high number of HSCTs each year and the significant morbidity associated with GVHD, there is significant market potential for a transformational GVHD therapeutic. Why do you believe cell therapies hold the answer?
If there is a small molecule or a biologic that does the job, then that conventional therapeutic will clearly be the preferred method of treatment. Therefore, the target product profile for any new product based on the technology of stem cells needs to exhibit dramatically superior efficacy attributes or safety attributes, or both. Consider some of the fundamentals of HSCTs: there is an increasing number of HSCTs performed worldwide, particularly allogeneic, and imperfectly HLA-matched allogeneic transplantations translate into a high incidence of GVHD of about 50%. Some GVHD patients can be treated using conventional therapies in the first line, but some are refractory to advanced GVHD biologics treatments, and unfortunately the current situation is that these non-responders essentially have no hope. That’s why finding new therapies, whether stem cells or other emerging pharmaceutical modalities such as nucleic acids, is important.
Stem cells exhibit the right attributes for complex indications, particularly mesenchymal stem cells (MSCs) or regulatory T cells (Tregs). MSCs because they have anti-inflammatory properties that help trigger a new type of response: they sense and respond to the environment, home to the site of inflammation and secrete an array of paracrine factors, which will ultimately help manage the inflammation. Tregs because they maintain peripheral tolerance and inhibit autoimmune responses as well as pathogenic tissue damage. Those are the basic mechanisms by which GVHD patients could receive novel clinical benefits. In a way, these novel treatments are akin to both a polypharmacy approach and to a personalized medicine approach. There is therefore a tremendous window of opportunity to derive clinical benefit for no-hope patients who do not respond to existing therapeutics.
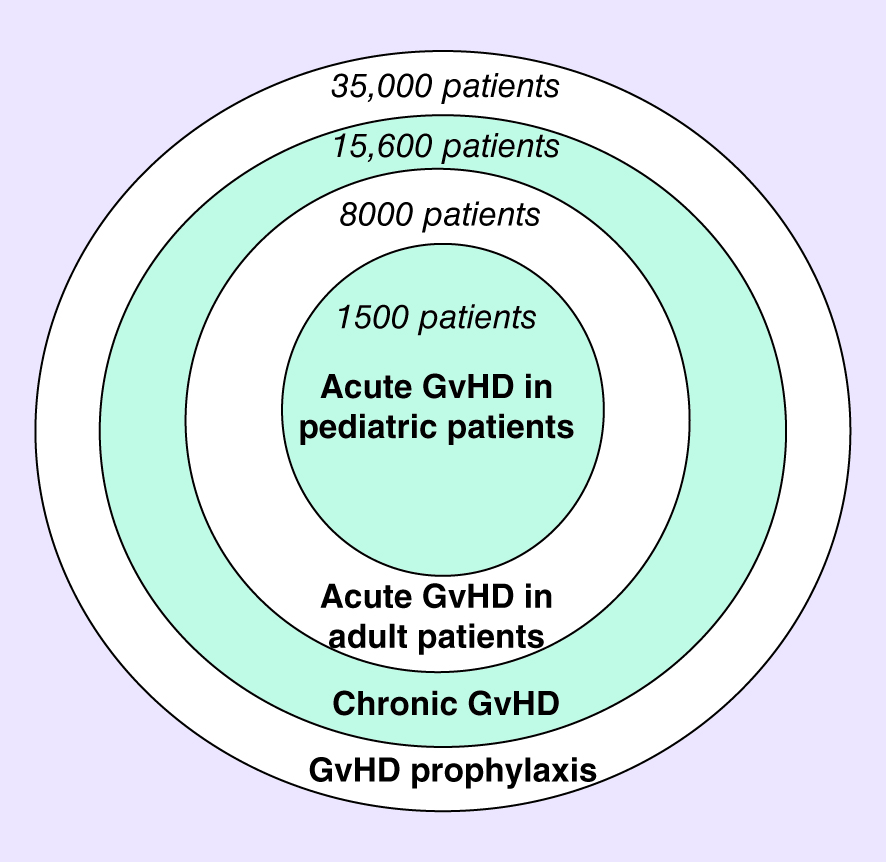
Market transformation map for a transformational graft-versus-host disease treatment. Originally appeared in ‘The potential of cytotherapeutics in hematologic reconstitution and in the treatment and prophylaxis of graft-versus-host disease. Chapter I: current practice and remaining unmet medical needs’, reproduced from Regen. Med. (2015) 10(3), 331—343 with permission of Future Medicine Ltd.
There are many MSC products under development for treating or preventing GVHD. Are there any that you feel particularly optimistic about?
There are different types of MSCs with some variations in manufacturing, surface markers and so on, and at the end of the day I don’t know which one is going to be the best preparation. Osiris Therapeutics Mesoblast acquired Osiris’s culture-expanded MSC business in 2013) was the first company developing MSCs for GVHD. This product, remestemcel-L, is well advanced in its clinical development for treating acute biologics-refractory pediatric GVHD, could potentially be the first globally commercialized cytotherapy for treating GVHD. Already, this product has been conditionally approved in Canada and New Zealand in 2012 for pediatric biologics-refractory acute GVHD; and in 2015 Mesoblast’s licensee in Japan, JCR Pharmaceuticals, received full approval by Japan’s Pharmaceuticals and Medical Devices Agency for its product, TEMCELL HS. Inj. , both pediatric and adult acute GVHD.
From a commercial consideration, having the first product on the market is critical. If you look again at the adoption of technologies, and particularly pharmaceutical products, the first-in-class products usually capture most of the market. On the other hand, a best-in-class product commercialized 2—5 years after the first-in-class product may capture only 40% of the market, so there is a tremendous advantage in being first. What’s more, from a patient consideration, it’s obviously critical to have this type of product available as soon as possible.
How do you think MSCs could be developed further as a potential therapy?
Let’s look at cytotherapies in general. The first time people in the field decided to make use of them, the first point of entry was to use autologous stem cells; that is, stem cells derived from the patient. This was done for ethical reasons and to avoid the risk of rejection or infectious contagions. However, an autologous point of entry doesn’t really fit the business models of traditional pharma built around blockbuster products manufactured at mass scales, and doesn’t fulfil either the needs of the majority of patients. Besides, cells from a patient carrying a genetic disease or from an older patient might not be as efficacious as cells sourced from a young healthy donor. The second wave of innovation in cytotherapeutics was thus to try allogeneic products, and reach the higher number of patients with cells produced at large scales and controlled for quality. At present, those cells so far have not yet been modified in any way, they are simply expanded ex vivo and minimally manipulated.
The next level is to attempt to take cell preparations and enhance their efficacy attributes. This goal can be achieved very simply by using different manufacturing techniques for example, and some companies are already working in this area. For instance, the simple variation of a discrete number of specific very basic manufacturing parameters, or even a single one, could suffice to produce cells of different metabolic states, resulting in cytotherapeutics enhanced for particular indications. This approach is already emerging. Some companies are working to provide totally new attributes to cells using even more complex techniques than a simple amendment to a manufacturing protocol, such as by enhancing the levels of the ligand CXCR4, which is expressed on the surface of MSCs and is important for the homing process. Similarly, one can elevate the concentration of chemoattractants like SDF-1 at the site of injury where you want the cells to act; or modify the surface of the cells ex vivo so they are coated with residues to assist homing. And again you can deliver some additional benefits to patients by using these new technologies, so by anticipating those S-curves of industry development, one can already anticipate the increased efficacy attributes that can be conferred to MSC preparations. Better efficacy means greater adoption by pharma and by practicing clinicians, and better patient benefits.
What other cell types or technologies might help suppress GVHD?
Recently there has been some interest in Tregs to help manage GVHD, with some clinical trials with Tregs taking place. We don’t yet know whether Tregs would be a better product than MSCs; we need to have more data. Nevertheless, it’s a very promising approach, and at the end of the day, the availability of different types of cytotherapies will enable clinicians to choose what treatment is best suited to treat a patient.
“…the availability of different types of cytotherapies will enable clinicians to choose what treatment s best suited to treat a patient.”
Looking to the future, what changes do you expect to see in the HSCT field in the next few years?
GVHD is clearly the main adverse event associated with HSCT. This risk is reducing the number of HSCTs but especially in those aged above 55 years who might experience higher morbidity and mortality resulting from myeloablative conditioning regimens. So, having a transformational product like an MSC or a Treg preparation that is safe and efficacious and that will help manage or even prevent the GVHD effects could result in an increase in the number of HSCTs worldwide making use of third party HSCs, as more patients who need them would receive them. Moreover, patients could perhaps undergo HSCT earlier in the disease rather than later, which could perhaps change the prognosis in some cases. Also, with subsequent clinical validations and eventually further improvements, we could very well see an evolution from the treatment of biologics-refractory pediatric acute GVHD, to the prevention of GVHD. An effective treatment for a clinically challenging condition like GVHD would be a win for the entire stem cell therapeutic industry, and this win would definitely promote their large-scale adoption. Similar to rituximab in the field of monoclonals, such a win would unambiguously and definitely prove the concept of cytotherapy: scientifically, technically, clinically and commercially.
“…we could very well see an evolution from the treatment of biologics-refractory pediatric acute GVHD, to the prevention of GVHD ….”
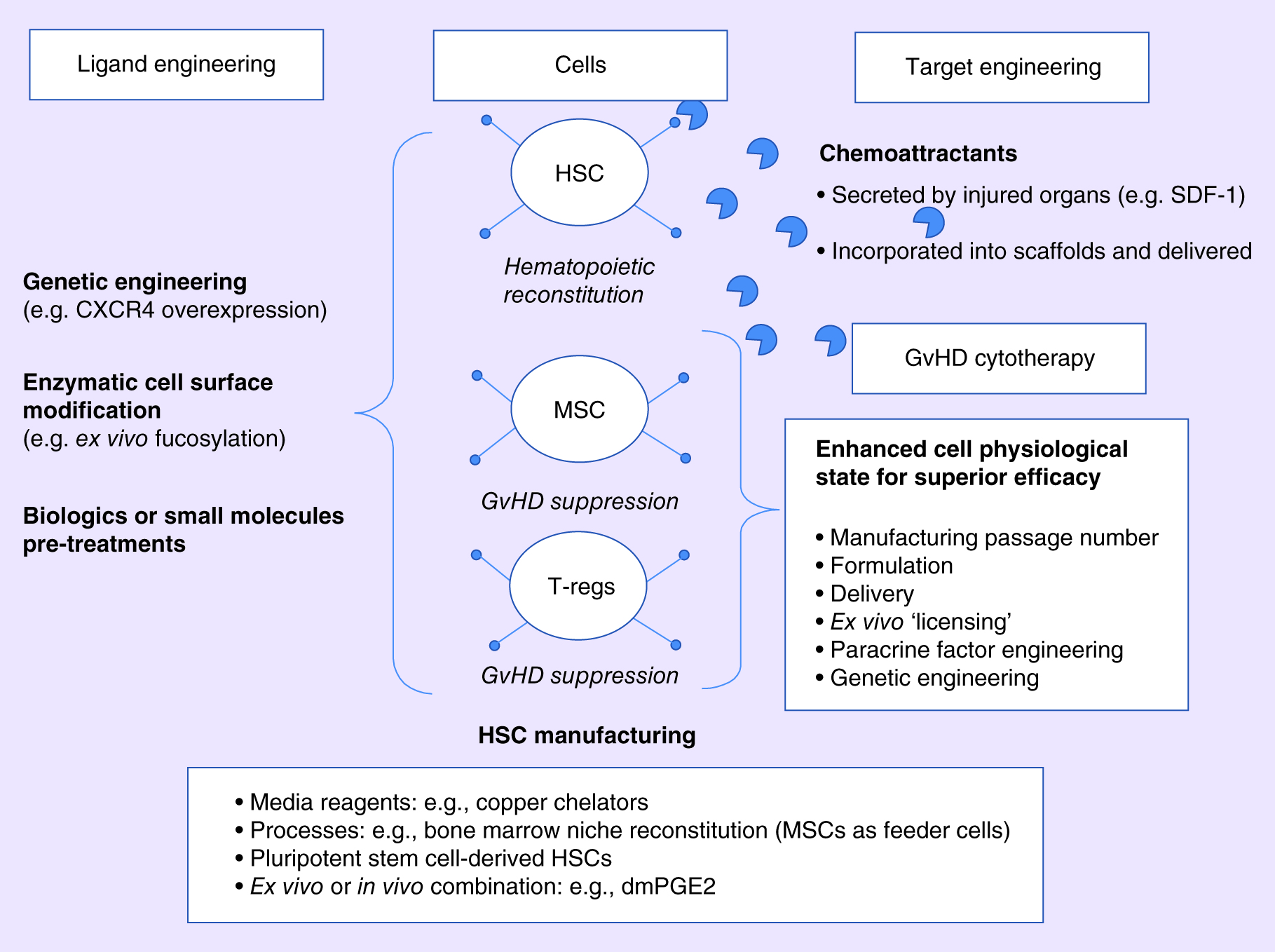
Various technologies in development for improving allo-hematopoietic stem cell transplantation. Originally appeared in ‘The potential of cytotherapeutics in hematologic reconstitution and in the treatment and prophylaxis of graft-versus-host disease. Chapter II: emerging transformational cytotherapies’, reproduced from Regen. Med. (2015) 10(3), 345—373 with permission of Future Medicine Ltd.
Further reading
Find Alain’s recent Regenerative Medicine review articles discussing the potential of cytotherapeutics in hematologic reconstitution and in the treatment and prophylaxis of GvHD below:
- The potential of cytotherapeutics in hematologic reconstitution and in the treatment and prophylaxis of graft-versus-host disease. Chapter I: current practice and remaining unmet medical needs
(Original publication date: 01/05/2015, Regenerative Medicine) - The potential of cytotherapeutics in hematologic reconstitution and in the treatment and prophylaxis of graft-versus-host disease. Chapter II: emerging transformational cytotherapies
(Original publication date: 01/05/2015, Regenerative Medicine)
Financial & competing interests’ disclosure
Alain Vertès discloses that, among the companies cited herewith, he has financial involvement with Mesoblast (Melbourne, Australia) and Targazyme (TX, USA).