huCART19-IL18: enhancing CAR-T cell therapy for blood cancers
A strategy enhancing CAR T-cells has demonstrated promising results in treating B-cell lymphoma.
A team of researchers at the Perelman School of Medicine at the University of Pennsylvania (PA, USA) previously developed a new anti-CD19 “armored” CAR T-cell therapy to enhance antitumor activity. Now, in a recent study involving a small cohort of B-cell lymphoma patients, the team has reported encouraging results, offering hope to patients with lymphoma where previous CAR-T therapy has been unsuccessful.
CAR-T cell therapy, a personalized cancer immunotherapy, utilizes a patient’s own T-cells that are modified ex vivo to recognize and attack cancer cells. Currently, four out of the seven CAR T-cell therapy products approved by the US Food and Drug Administration (FDA; MD, USA) are indicated to treat B-cell lymphomas. However, more than 50% of lymphoma patients who have received the current available CAR-T therapy do not have long-term remission. This can be due to immune suppression or T-cell exhaustion that can limit the effectiveness of subsequent CAR-T administrations after an initial treatment. This results in limited treatment options for returning or resistant cancers.

FDA-approved cell and gene therapies
This overview examines the cell and gene therapies that are currently FDA-approved, offering new possibilities for patients worldwide.
To address these limitations, Carl June and his team, the pioneers of CAR-T cell therapy, have now enhanced their CAR-T platform by engineering the cells to secrete interleukin 18 (IL18), a proinflammatory cytokine, yielding huCART19-IL18 – the “armored” CAR-T. huCART19-IL18 targets the surface antigen CD19 – like most CAR T-cell products; however, the addition of IL18 secretion enables the recruitment of more immune cells to support the modified T cells. This modification intends to strengthen the protection of CAR T-cells and promote their ability to attack cancer cells, overall enhancing anti-tumor activity.
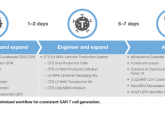
Additionally, the production of huCART19-IL18 uses a 3-day manufacturing process developed by the University’s Center for Cellular Immunotherapies, significantly shorter than the traditional 9–14-day period. This significant reduction in manufacturing time is particularly crucial for patients battling aggressive, rapidly progressing cancers, as it allows them to start their CAR T-cell treatment much sooner.
Assessing their cytokine-enhanced CAR-T strategy, the first of its kind tested in blood cancer patients, the researchers conducted a small Phase I trial involving 21 patients with B-cell lymphomas where cancer treatment, including commercially available CAR T-cell therapies, had been ineffective. After the patients received the treatment, in doses ranging from 3×106 to 3×108, the team analyzed blood samples to assess immune response rates.
Three months after the initial huCART19-IL18 infusion, 81% of patients had a complete or partial response and 52% of patients had complete remission. They observed robust CAR T-cell expansion across all dose levels with no unexpected adverse effects. Sixty-two percent of patients did however, experience cytokine release syndrome and 14% of patients had immune effector-cell–associated neurotoxicity – common side effects of CAR-T therapy. Encouragingly, the researchers reported that some patients treated earlier in the study experienced durable remission for two years or more.
“Based on these results, we believe that incorporating cytokine secretion into CAR T-cell design will have broad implications for enhancing cellular therapies, even beyond blood cancers,” June said. “With longer T-cell persistence and expansion, this strategy could be powerful in settings where CAR-T hasn’t performed as well, such as solid tumors.”
The researchers plan to conduct other clinical trials, including expanding huCART19-IL18 to acute and chronic lymphocytic leukemia patients. The team is also actively enrolling non-Hodgkin’s lymphoma patients to assess a similar IL18-armored CAR T-cell product.
“We know that bringing this type of new therapy from the lab bench to the patient bedside is only possible at a place like Penn Medicine, thanks to our courageous patients and the teamwork between our scientific and clinical teams,” expressed Jakub Svoboda, who led the study. “With the biopsies and cytokine data from this trial, we’ve gained a wealth of information about patients relapsing after CAR-T cell therapy that could help researchers better understand the science of CAR-T cell therapy relapse in general.”
Furthermore, the team have partnered with a spinout company of the university to improve the process of the ex vivo production and expansion of huCART19-IL18 before treatment administration, as previous research has indicated that reducing the manufacturing time of CAR-T cells may enhance T-cell potency.