How Treg cells impact CAR-T therapy: insights from the Cancer Correlative Science Unit
Diving into the intricate world of CAR-T cell therapy, Bita Sahaf shares insights from her work at the Cancer Correlative Science Unit in the Stanford Center for Cancer Cell Therapy (CA, USA). In this interview, Dr Sahaf discusses the practical aspects of biomarker discovery, patient-specific variability and potential strategies to enhance CAR-T efficacy by addressing Treg-mediated suppression.
Questions
The Cancer Correlative Science Unit (CCSU) was established to serve as an integral component of the Stanford Center for Cancer Cell Therapy. Our working model employs an iterative cycle of translational research, where basic science, manufacturing, clinical, correlative science, and data science teams work in collaboration. The CCSU conducts patient-focused discovery research as part of this iterative cycle of translational science. By working with translational scientists throughout the Center, the CCSU drives collaborations and innovation. CCSU team members are each specialist in their dedicated assay.
Science emanating from the CCSU spans fundamental biology, mechanisms of resistance and biomarker discovery. These data inform the next generation of CAR-T design. Cutting-edge multiomic assays have been designed, optimized and performed by CCSU, powering innovative biomarker discovery (Figure 1).
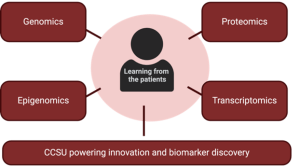
Figure 1. Single-cell level multiomic assays optimized and performed at CCSU.
Good et al. provide the first example of biomarker discovery leveraging the CCSU infrastructure [1]. By leveraging a combination of mass cytometry and machine learning data analyses on standardized assays produced in CCSU, our team identified metaclusters of circulating lymphocyte populations associated with high rates of durable disease control and neurotoxicity in patients receiving Axi-cel for diffuse large B cell lymphoma. Higher levels of the metacluster of CD4+ CAR-T cells expressing Helios and CD25 was associated with a higher risk of disease progression and a lower risk of neurotoxicity after CD19-CAR treatment. These cells were non-clonal and displayed a Treg cell phenotype, also expressing FOXP3.
We have shown that in the specific case mentioned above, the Treg-like cells were suppressive for CAR-T function and thereby diminished the expansion of effector CAR-T cells, limiting both antitumor effects and cytokine-mediated neurotoxicity. Work is ongoing in the context of other CAR-T cells for large B cell lymphoma and for CAR-T cells treating other diseases.
Our data has shown that these Tregs are by themselves markers of a higher risk of progression. Although we have been relying on complex mass cytometry assays to find this biomarker, now that we have described the metacluster we are studying this more widely using high-dimensional flow cytometry, widely available in clinical diagnostic settings and in hospitals.
Flow cytometry is a powerful tool when used correctly. Powerful high-dimensional panels are designed to investigate this biomarker in a wide variety of diseases treated with CAR-T cells.
Although I have been discussing Treg-like cells as biomarkers for higher risk of progression in studies utilizing flow and mass cytometry, we have been using a variety of assays to corroborate and study different types of specimens and we have discovered additional biomarkers of CAR-T function and expansion. Combining flow cytometry with CITE-Seq (Cellular Indexing of Transcriptomes and Epitopes by Sequencing) and scRNA-Seq (single-cell RNA sequencing) is a great way of discovering cell phenotypes as biomarkers.
For instance, CAR-T copy number assessment by qPCR and ddPCR assays measuring Histone-3 mutation levels in the cerebrospinal fluid of CAR-T-treated diffuse intrinsic pontine glioma patients are also proving to be biomarkers of response to therapy [2].
In a separate study, we discovered that in a cohort of pediatric patients treated with CAR-T cells that target the disialoganglioside GD2 expressed on tumor cells, the epigenetic differences in patients’ T cells in peripheral blood samples obtained before any CAR-T manufacturing and therapy serve as a biomarker for good or poor CAR-T cell expansion [3].
Since biopsies are not always attainable after therapy, for example, after diffuse intrinsic pontine glioma and diffuse midline glioma CAR-T therapy, scRNA-Seq and CITE-Seq analysis of the limited cells isolated from cerebrospinal fluid in patients has proven to be very important to gain insight into brain tumor CAR-T therapy. Cell surface protein libraries combined with powerful transcriptome libraries provide insight into cell phenotype and functional states combining both proteomic and transcriptome information.
This remains to be studied, however, there are certain conditions that are associated with increased levels of circulating Tregs. We hypothesize that pre-treatment levels may affect the outcome of therapy after autologous CAR-T cell therapy.
Since autologous CAR-T cells are produced by transducing patients’ own T cells, the condition, function, and phenotype of their cells is bound to directly influence how functional the resulting CAR-T cells will be.
This is being studied by many groups, as there appears to be a direct association between the lines of therapy received prior to CAR-T treatment and the quality and functionality of the CAR-T in the patients. Our research has demonstrated that greater stemness of T cells before CAR-T cell production is associated with improved functionality of the CAR-T cells following infusion [1].
One potential approach is employing high-dimensional sorting to remove Tregs before attempting to transduce the T cells with the CAR-T construct. Whether it is feasible to scale this remains to be seen. Possibly utilizing GMP-grade flow cartridges that can accommodate negative selection of cells would offer a scalable solution.
Meet the interviewee
 Bita Sahaf, Director, Stanford Cancer Correlative Science Unit, Stanford Cancer Institute
Bita Sahaf, Director, Stanford Cancer Correlative Science Unit, Stanford Cancer Institute
Bita Sahaf is a translational scientist studying the pharmacodynamics of immune-modulatory drugs, checkpoint inhibitors and CAR-T therapies in clinical trials. Dr Sahaf received her PhD from Linköping University (Sweden) in 2001 before beginning her postdoctoral research at the Herzenberg Laboratory in the Department of Genetics at Stanford University School of Medicine (CA, USA). Presently, Dr Sahaf is the Director of the Cancer Correlative Science Unit at the Stanford Cancer Institute (CA, USA).
Disclaimer
The opinions expressed in this interview are those of the author and do not necessarily reflect the views of RegMedNet or Taylor & Francis Group.
In association with

![]()